At CSIBW, we are dedicated to delivering healthcare services to underserved rural communities, ensuring that even the most remote populations have access to preventive and primary care. Through mobile public health camps, we provide essential health services, raise awareness about nutrition, sanitation, and lifestyle diseases, and collaborate closely with health professionals and local bodies to maximize the impact of our outreach.
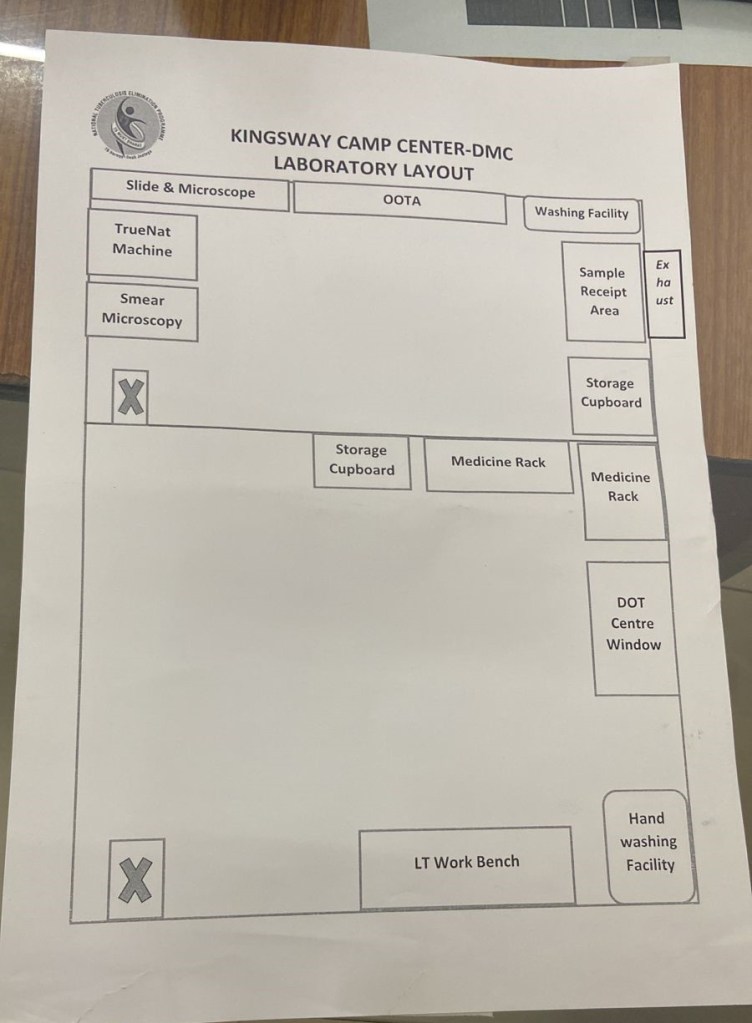
Optimizing TB Laboratory Layout as part of QMS Implementation
Quality Management Systems (QMS) for TB laboratories
We have published work on Quality Management Systems (QMS) for TB laboratories. QMS is considered a “sine qua non” for patient management, as weak systems can lead to under- or over-diagnosis of TB, unnecessary anti-TB treatment, and delayed reporting; all of which negatively impact patient care. By standardizing laboratory procedures, monitoring performance, and maintaining strict quality control, QMS enhances diagnostic precision, strengthens health systems, and improves patient outcomes. Continuous quality improvement based on QMS principles ensures accuracy, reliability, cost-effectiveness, and long-term sustainability of public health programs, reinforcing both laboratory service quality and overarching patient management.

Screening Construction Workers for Tuberculosis
Tuberculosis, health knowledge, risk perception, and coping behaviors among migrant construction workers, Bangalore, Karnataka, India
CSIBW has established the prevalence of Tuberculosis, health knowledge, risk perception, and coping behaviors among migrant construction workers in Bangalore Urban. High vulnerability to TB was largely due to poor living and working conditions, low awareness of government health services, treatment non-adherence, and frequent migration. By embedding TB control within the everyday realities of construction sites, policymakers and stakeholders we can both improve the health and quality of life of workers and contribute meaningfully to India’s goal of TB elimination. Our educational efforts created awareness of work-related safety and health issues in this population.

Screening e-Rickshaw Drivers for Tuberculosis
Prevalence of Tuberculosis and Latent TB infection and its associated factors among rickshaw drivers, New Delhi, India
TB diagnosis is generally delayed when health seeking behavior is postponed after the onset of symptoms. This generates immense human and economic loss, and it is now become the utmost task for health system to focus on resources to diagnose and tackle this behavior. Active case TB finding led to the detection of additional TB cases in rickshaw drivers in Delhi where no TB cases were detected prior to this activity. We contributed towards early case finding, treatment initiation in a particular vulnerable group and thus improving health sequelae and social and economic consequences of TB. We demonstrated that screening of rickshaw drivers for TB and latent TB Infection is a feasible and efficient tool that can potentially result in early diagnosis and treatment of active TB, thus minimizing the disease severity and decreasing TB transmission.
India’s Pradhan Mantri TB Mukht Bharat Abhiyan to engage communities is a great initiative in the right direction which will create bio-social model approach to stopping TB. It not only aims to target morbidity and mortality from the disease but would also contribute substantially to poverty alleviation and sustainable development that promises to meet the health needs of high-risk population including migrants.

Setting up TB Diagnostics at Jso-Jey Clinic, Rumtek Monastery, SIkkim
Tuberculosis and latent TB infection (TBI) in congregate setting in a monastery at Gangtok, Sikkim, India
Sikkim is home to several Buddhist monasteries where students/monks from diverse and faraway places visit. These monks are frequent travelers and therefore happen to be at risk of TB exposure, which makes them potential transmitters of disease outside of the monasteries. We published work on high prevalence of TB and TBI among residents in the congregate setting of Rumtek monastery that justify TB prevention strategies by targeted screening, TBI testing and preventive treatment.
Increasing age, abnormal BMI, a history of tuberculosis and frequent travel heightened vulnerability of individuals in monastic environments due to close living quarters, communal activities, and frequent mobility. We presented a compelling case for the National TB Elimination Program (NTEP) to develop targeted interventions for monasteries and similar congregate settings focusing on high-risk populations to prevent TBI progression to active TB disease.
